Systemic Mastocytosis

Mastocytosis is often referred to as mast cell disease
Systemic mastocytosis (SM) is a form of mastocytosis in which mast cells accumulate in internal tissues and organs such as the liver, spleen, bone marrow, and small intestines. It is typically diagnosed in adults. Signs and symptoms vary based on which parts of the body are affected. The ICD-10 code for systemic mastocytosis is “D47.02“.
To keep us healthy, mast cells protect our body from foreign threats, such as infections, and help repair its tissues once the threat is gone. As part of their role in the immune system, they create histamine — neurotransmitters that react to those threats and allergens, such as bee stings. Histamine is also released in response to allergens, causing reaction symptoms such as inflammation and even anaphylaxis, a severe, potentially life-threatening kind of reaction.
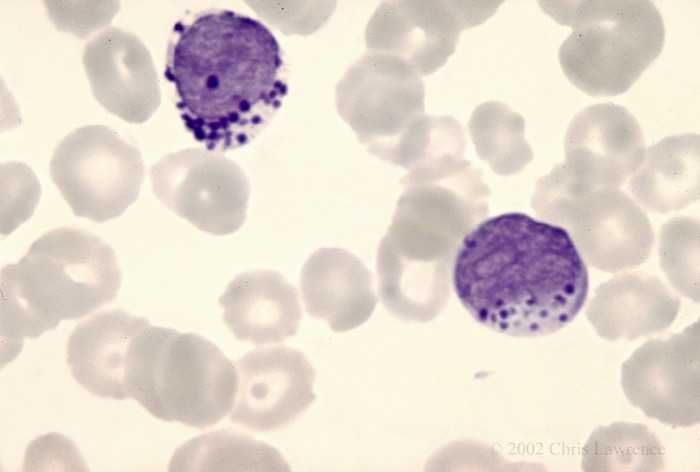
Mast cell leukemia – Peripheral Blood
Mastocytosis is caused by a genetic mutation in which the body accumulates too many mast cells — white blood cells that are part of the immune system and help fight infections.
The World Health Organization (WHO) classification of mastocytosis includes the following:
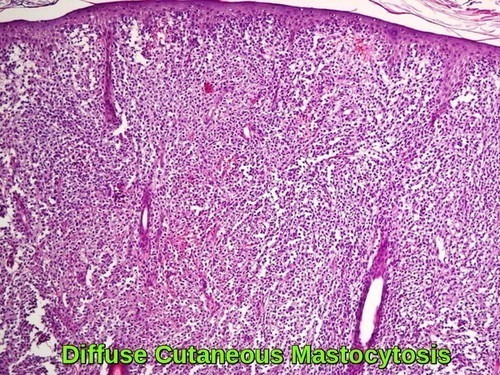
- Cutaneous mastocytosis – Urticaria pigmentosa, maculopapular cutaneous mastocytosis, diffuse cutaneous mastocytosis, mastocytoma of skin. Cutaneous mastocytosis mainly affects children – where mast cells gather in the skin but are not found in large numbers elsewhere in the body
- Indolent systemic mastocytosis.
- Systemic mastocytosis with an associated (clonal) hematologic non–mast cell lineage disease.
- Aggressive systemic mastocytosis.
- Mast cell leukemia.
- Mast cell sarcoma.
- Extracutaneous mastocytoma.
Mast cells:
Mast cells are produced in the bone marrow, the spongy tissue found in the hollow centers of some bones, and live longer than normal cells. They’re an important part of the immune system and help fight infection.
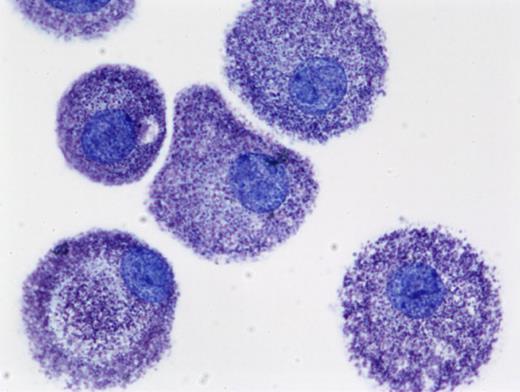
Human mast cells cultured from peripheral blood in SCF (stem cell factor) and stained with toluidine blue(cytoprep; 400×). The figure is provided courtesy of Madeleine K. Radinger.
When mast cells detect a substance that triggers an allergic reaction (an allergen), they release histamine and other chemicals into the bloodstream.

Histamine makes the blood vessels expand and the surrounding skin itchy and swollen. It can also create a build-up of mucus in the airways, which become narrower.
Symptoms of mastocytosis:
The symptoms of mastocytosis can vary depending on the type.
Cutaneous mastocytosis
The most common symptom of cutaneous mastocytosis is abnormal growths (lesions) on the skin, such as bumps and spots, which can form on the body and sometimes blister. The spots are thick and itch when they are hot or if rubbed over it. These spots are known as urticaria pigmentosa.

Systemic mastocytosis
Some people with systemic mastocytosis may experience episodes of severe symptoms that last 15-30 minutes, often with specific triggers such as physical exertion or stress. Many people do not have any problems.
During an episode you may have:
- skin reactions – such as itching and flushing
- gut symptoms – such as being sick and diarrhea
- muscle and joint pain
- mood changes, headaches, and episodes of tiredness (fatigue)
People with mastocytosis have an increased risk of developing a severe and life-threatening allergic reaction. This is known as anaphylaxis.
The increased risk of anaphylaxis is caused by the abnormally high number of mast cells and their potential to release large amounts of histamine into the blood.
People with mastocytosis may need to carry an adrenaline auto-injector, which can be used to treat the symptoms of anaphylaxis.
There are 3 subtypes of systemic mastocytosis:
- indolent mastocytosis – symptoms are usually mild to moderate and vary from person to person; indolent mastocytosis accounts for around 90% of adult systemic mastocytosis cases.
- aggressive mastocytosis – where mast cells multiply in organs, such as the spleen, liver and digestive system; the symptoms are more wide-ranging and severe, although skin lesions are less common.
- systemic mastocytosis with associated hematological disease – where a condition that affects the blood cells, such as chronic leukemia, also develops.
Causes of mastocytosis:
The cause or causes of mastocytosis are not fully known, but there’s thought to be an association with a change in genes known as the KIT mutation.
The KIT mutation makes the mast cells more sensitive to the effects of a signaling protein called stem cell factor (SCF).
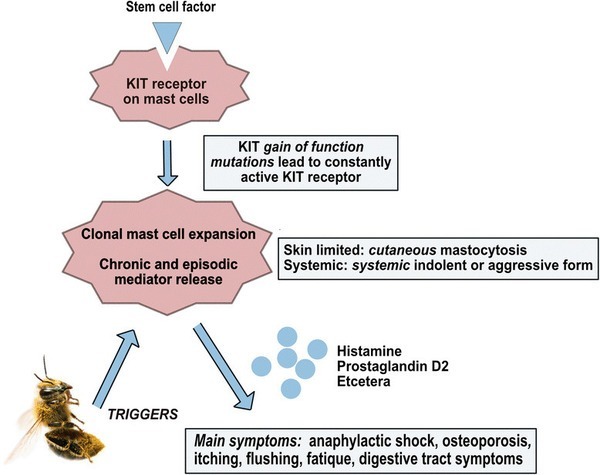
SCF plays an important role in stimulating the production and survival of certain cells, such as blood cells and mast cells, inside the bone marrow.
In very few cases of mastocytosis, it appears the KIT mutation is passed down through families. However, in most cases, the mutation happens for no apparent reason.
Diagnosing mastocytosis:
A physical examination of the skin is the first stage in diagnosing cutaneous mastocytosis.
Your child’s GP or a skin specialist (dermatologist) may rub the affected areas of skin to see if they become red, inflamed and itchy. This is known as Darier’s sign.

Darier’s sign is an important dermatological finding and may be elicited by stroking a mastocytosis skin lesion approximately 5 times with moderate pressure with a tongue spatula. Within a few minutes, a wheal and flare reaction of the lesion develops (arrow).
It’s usually possible to confirm a diagnosis by carrying out a biopsy, where a small skin sample is taken and checked for mast cells.
The following tests are commonly used to look for systemic mastocytosis:
- blood tests – including a full blood count and measuring blood tryptase levels
- an ultrasound scan to look for enlargement of the liver and spleen
- a DEXA scan to measure bone density
- a bone marrow biopsy test – where a local anesthetic is used and a long needle is inserted through the skin into the bone underneath, usually in the pelvis
A diagnosis of systemic mastocytosis is usually made by finding typical changes on a bone marrow biopsy.
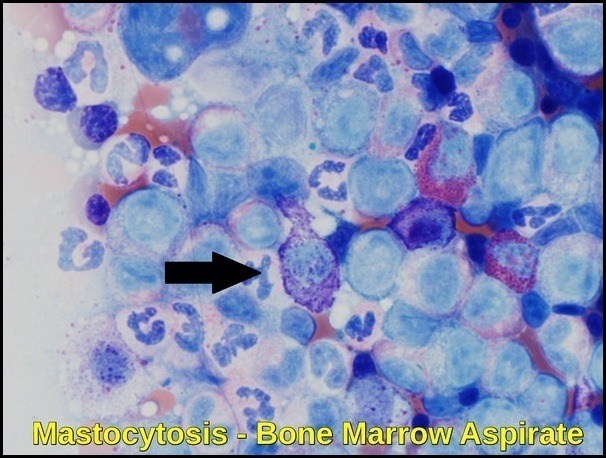
Neoplastic spindle-shaped mast cell with an elongated cytoplasmic projection. The cell is enlarged and the cytoplasm is hypogranular compared to normal mast cells. Wright Giemsa stain, 100X.
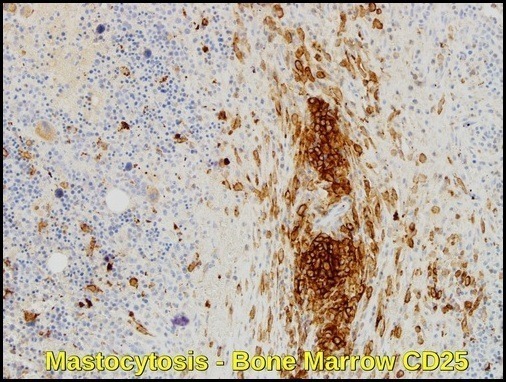
This bone marrow biopsy from a 61-year-old man with indolent systemic mastocytosis shows a large mast cell aggregate surrounding a blood vessel. The brown stain is an antibody directed against CD25, the interleukin 2 receptor, which highlights neoplastic but not normal mast cells. The compact cluster of mast cells has many round cells, but toward the edges of the aggregate, they appear spindle-shaped. CD25 immunohistochemical stain, 20X.
Diagnostic Criteria:
The single World Health Organization (WHO) major criterion is multifocal dense infiltrates of mast cells in the bone marrow and/or other extracutaneous organs. One major and 1 minor criterion or 3 minor diagnostic criteria are needed to establish a diagnosis of systemic mastocytosis.
Minor criteria include baseline total tryptase level of greater than 20 ng/mL; greater than 25% of the mast cells in bone marrow aspirate smears or tissue biopsy sections having spindle atypical morphology; mast cells in bone marrow, blood, or other lesional tissue expressing CD25 or CD2; or detection of a codon 816 c-kit point mutation in blood, bone marrow, or lesional tissue.
Treatment:
The treatment of mastocytosis depends on the type, the symptoms of the disease, its extent, and the person’s overall health.
There is no cure for mastocytosis, although several treatments can be used to relieve symptoms and remove a mastocytoma.
Managing symptoms
An important part of treating mastocytosis is controlling a person’s symptoms. One important way to do this is to avoid anything that may cause mast cells to release histamine. This may include extreme temperatures, alcohol, emotional stress, insect bites, and certain medications. For example, nonsteroidal anti-inflammatory drugs (NSAIDs) should be used with caution because these drugs may trigger the release of histamine and can cause severe reactions or an attack.
Doctors may also recommend the following treatments to help relieve mastocytosis symptoms.
Antihistamines. Antihistamines help relieve itching, flushing, and other skin reactions.
Steroids. Steroids may be used to reduce the size of skin lesions.
Epinephrine. People with mastocytosis often carry a syringe of epinephrine, a hormone made by the adrenal glands, in case they need to treat a severe allergic reaction.
Other medications. Other medications can help relieve diarrhea and stomach pain.
Ultraviolet light. Sometimes, exposing the skin rashes to a source of ultraviolet (UV) light can help relieve symptoms of cutaneous mastocytosis.
Surgery. surgery may be performed to remove lesions, such as a mastocytoma.
Targeted therapy. targeted therapy is a treatment that targets the disease’s specific genes, proteins, or the tissue environment unique to mastocytosis that contribute to its growth and survival. This type of treatment blocks the growth of mast cells while limiting damage to healthy cells. Tyrosine kinase inhibitors are a type of targeted therapy. For mastocytosis, the target is the unique protein called the c-kit tyrosine kinase receptor. Treatment with tyrosine kinase inhibitors, including dasatinib (Sprycel), midostaurin (PKC412, recently approved by the FDA for the treatment of systemic mastocytosis), and less commonly imatinib (Gleevec) and nilotinib (Tasigna), may be considered for patients with mast cells that have a mutation in the c-kit tyrosine kinase receptor.
Avapritinib (Ayvakit), a highly selective inhibitor of KIT D816V, was approved by the Food and Drug Administration in 2021 for treatment of advanced systemic mastocytosis (AdvSM) and by the European Medicines Agency in 2022 for AdvSM after prior systemic therapy. The phase 1 EXPLORER and phase 2 PATHFINDER trials demonstrated that avapritinib can elicit complete and durable clinical responses and molecular remission of KIT D816V.

AYVAKIT™ (avapritinib) is the first precision therapy approved for the treatment of adults with unresectable or metastatic gastrointestinal stromal tumours (GISTs) and advanced systemic mastocytosis (ASM).
Stem cell transplantation/bone marrow transplantation
A stem cell transplant is a medical procedure in which unhealthy bone marrow is replaced by highly specialized cells, called hematopoietic stem cells, that develop into healthy bone marrow. Hematopoietic stem cells are blood-forming cells found both in the bloodstream and in the bone marrow. Today, this procedure is more commonly called a stem cell transplant, rather than bone marrow transplant, because it is the stem cells in the blood that are typically being transplanted, not the actual bone marrow tissue.
Before recommending transplantation, doctors will talk with the patient about the risks of this treatment and consider several other factors, such as the results of any previous treatment and the patient’s age and general health.
There are 2 types of stem cell transplantation depending on the source of the replacement blood stem cells: allogeneic (ALLO) and autologous (AUTO). ALLO uses donated stem cells, while AUTO uses the patient’s own stem cells. In both types, the goal is to destroy all unhealthy cells in the marrow, blood, and other parts of the body using high doses of chemotherapy and/or radiation therapy and then allow replacement blood stem cells to create healthy bone marrow.
Stem cell transplantation is not used frequently as a treatment for mastocytosis because treatment results are inconsistent and there are significant risks associated with this treatment approach.
Chemotherapy for mastocytosis-related cancer
Chemotherapy is sometimes recommended if mastocytosis becomes cancerous. Chemotherapy is the use of drugs to destroy cancer cells, usually by ending the cancer cells’ ability to grow and divide.
Systemic chemotherapy gets into the bloodstream to reach cancer cells throughout the body. Common ways to give chemotherapy include an intravenous (IV) tube placed into a vein using a needle or in a pill or capsule that is swallowed (orally).
A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A patient may receive 1 drug at a time or combinations of different drugs given at the same time.
The side effects of chemotherapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, hair loss, loss of appetite, and diarrhea. These side effects usually go away after treatment is finished.
Getting care for side effects
Mastocytosis treatment often causes side effects. In addition to treatment to manage the condition, an important part of treatment is relieving these side effects. This approach is called palliative or supportive care, and it includes supporting the patient with his or her physical, emotional, and social needs.
Palliative care is any treatment that focuses on reducing symptoms and treatment side effects, improving quality of life and supporting patients and their families. Any person, regardless of age or type of disease, may receive palliative care. It works best when palliative care is started as early as needed in the treatment process.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional support, and other therapies.
Complications of Mastocytosis:
In children, the symptoms of cutaneous mastocytosis usually improve over time but remain stable in adults. In many cases, the condition gets better on its own by the time a child has reached puberty.
The outlook for systemic mastocytosis can vary, depending on the type.
Indolent systemic mastocytosis should not affect life expectancy, but other types can.
A few people develop a serious blood condition, such as chronic leukemia, over their lifetime.
Summary:
Systemic mastocytosis is a rare disorder characterized by abnormal growth and accumulation of mast cells in various tissues of the body. It can affect multiple organs, including the skin, bone marrow, liver, spleen, and gastrointestinal tract. The clinical presentation of systemic mastocytosis is highly variable and ranges from asymptomatic to life-threatening anaphylaxis.
The diagnosis of systemic mastocytosis is based on clinical, histopathological, and molecular criteria. The World Health Organization (WHO) classification system divides systemic mastocytosis into several subtypes based on the extent and severity of organ involvement.
Treatment options for systemic mastocytosis depend on the subtype and clinical presentation. Symptomatic management includes antihistamines, corticosteroids, and epinephrine for anaphylaxis. Targeted therapies, such as tyrosine kinase inhibitors, KIT D816V inhibitors, and monoclonal antibodies, are available for patients with advanced disease.
References:
Jacquiline Habashy, Dirk M Elston. Mastocytosis: Background, Pathophysiology, Etiology. https://emedicine.medscape.com/article/1057932-overview
Mastocytosis; overview, symptoms, and treatment. https://www.nhs.uk/conditions/mastocytosis/
Patnaik MM, Rindos M, Kouides PA, Tefferi A, Pardanani A. Systemic mastocytosis: a concise clinical and laboratory review. Arch Pathol Lab Med. 2007 May. 131(5):784-91.
Valent P. Diagnostic evaluation and classification of mastocytosis. Immunol Allergy Clin North Am. 2006 Aug. 26(3):515-34.
Horny HP, Sotlar K, Valent P. Mastocytosis: state of the art. Pathobiology. 2007. 74(2):121-32.
Dean D. Metcalfe; Mast cells and mastocytosis. Blood 2008; 112 (4): 946–956. doi: https://doi.org/10.1182/blood-2007-11-078097
Broesby-Olsen et al. Multidisciplinary Management of Mastocytosis: Nordic Expert Group Consensus. Acta dermato-venereologica. 96. 10.2340/00015555-2325.
Mastocytosis: What is It and How Is It Treated? | Dana-Farber Cancer Institute https://blog.dana-farber.org/insight/2017/12/mastocytosis-treatment/
Daniel Bustamante, MD and Tracy I. George, MD. Bone Marrow Biopsy Evaluation for Mast Cell Disorders. https://tmsforacure.org/expert-information/bone-marrow-biopsy-evaluation-mast-cell-disorders/
Mastocytosis: Treatment Options. https://www.cancer.net/cancer-types/mastocytosis/treatment-options
Systemic Mastocytosis. https://www.omicsonline.org/ireland/systemic-mastocytosis-peer-reviewed-pdf-ppt-articles/
Correcting Mast Cell Activation Syndrome – Histamine Intolerance – Mastocytosis https://biologixcenter.com/allergies/correcting-mast-cell-activation-syndrome-histamine-intolerance-mastocytosis/
Image of peripheral blood smear of acute mast cell leukemia. Wikipedia (2015). https://en.wikipedia.org/wiki/Mast_cell_leukemia. Accessed on December 2, 2015.
Jason GotlibAndreas ReiterDaniel J. DeAngelo; Avapritinib for advanced systemic mastocytosis. Blood 2022; 140 (15): 1667–1673. doi: https://doi.org/10.1182/blood.2021014612
AYVAKIT (avapritinib) for the Treatment of Gastrointestinal Stromal Tumours (GISTs) https://www.clinicaltrialsarena.com/projects/ayvakit-avapritinib/
Keywords:
Mastocytosis, mastocytosis symptoms, mastocytosis treatment, mastocytosis rash, mastocytosis diagnosis, mastocytosis symptoms in adults, mastocytosis photos, mastocytosis ICD 10, mastocytosis skin, mastocytosis cancer, mastocytosis symptoms child, mastocytosis symptoms adults, mastocytosis symptoms treatment, mastocytosis treatment update, mastocytosis treatment imatinib, mastocytosis treatment avapritinib, mastocytosis rash pictures, mastocytosis rash treatment, systemic mastocytosis rash, systemic mastocytosis rash pictures, mastocytosis diagnosis blood test, indolent mastocytosis diagnosis, indolent systemic mastocytosis diagnosis, aggressive systemic mastocytosis diagnosis, mast cell disease symptoms in adults, how do you know if you have mastocytosis.









Very nice informative and impressive post you have written, this is quite interesting and i have went through it completely, an upgraded information is shared, keep sharing such valuable information.
I am battling this right now. I have been sick for a very long time. But progressively worse in the past 6 months. Which is when my skin started displaying the symptoms and a dermatologist was finally able to identify it. Unfortunately, I am just now starting the systemic dx process and it could take awhile. With an upped dosage of my h1 and h2, adding singular, my rash is still uncontrollable and the brown spots are also starting to take over my body. I cannot find a lot of information about treating the skin and mixed information about if the spots and rash stay forever. Is there a more effective treatment to target these symptoms specifically? Will the spots stay forever? Should the itchyness and rash fade once I get stabalized with right medications? Unfortunately, I have not been able to come across many doctors who are well versed in mast cell disorders. So I am desperately researching and trying to reach out to anyone who can help.
Hi Kristin,
Thanks for your comment.
I totally understand your frustration caused by the itchiness and the disfiguring skin rash.
However, there is some piece of information missing in your comment regarding the diagnosis of systemic mastocytosis made by your dermatologist:
1- How high is your blood tryptase level?
2- Have you had an abdominal ultrasound scan?
3- Have you had a bone marrow biopsy?
4- Have you had a trial of systemic steroids?
Looking forward to having your answers to better understand and advise regarding your disease.
BW,
My wife, 66, was recently diagnosed with systemic mastocytosis. This article has been extremely helpful in preparing us for our first consult with a hemotologist. Many thanks Dr. Abdou.
Hi Jason,
Thank you for taking the time to reach out to me.
I really appreciate your kind words.
I also want to extend my best wishes to your wife for a speedy recovery.
Take care and all the best.
M Abdou