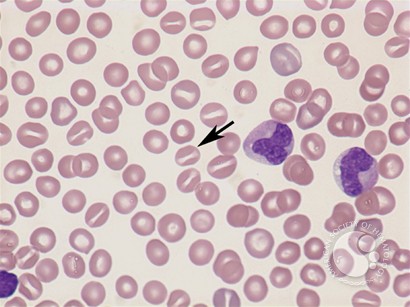
Stomatocytosis

Peripheral blood smear micrograph showing multiple stomatocytes (mouth-shaped red blood cells). This finding is characteristic of hereditary stomatocytosis, but can also be an acquired finding in liver disease, alcoholism, or certain drug exposures.
Stomatocytosis is a rare red blood cell (RBC) membrane disorder characterised by the presence of stomatocytes—red cells with a slit-like or mouth-shaped central pallor—on the peripheral blood smear. Hereditary stomatocytosis and acquired forms are associated with altered membrane permeability, hemolysis, and variable degrees of anemia. Recognition of stomatocytosis is important in hematology because it may indicate an underlying red cell membrane defect or systemic disease.

Normal red blood cell versus stomatocyte demonstrating the classic central slit of stomatocytosis.

Peripheral blood film highlighting stomatocytes with a central slit-like area of pallor, a hallmark finding in stomatocytosis.
Genetics & Molecular Pathophysiology:
Hereditary stomatocytosis is primarily associated with mutations in genes that regulate red blood cell (RBC) membrane permeability, including PIEZO1, RHAG, and ABCG5/8. These mutations alter cation transport, leading to abnormal hydration of RBCs. The disorder is usually inherited in an autosomal dominant pattern, though acquired stomatocytosis may develop secondary to alcohol misuse, liver disease, or certain medications. Genotype–phenotype correlation is variable, and molecular testing can support diagnosis in selected cases.
Laboratory Findings & Diagnosis:
Diagnosis of stomatocytosis is based on a combination of blood smear morphology and laboratory evidence of hemolysis.
Peripheral blood smear: In hereditary stomatocytosis, stomatocytes usually constitute 10–30% or more of circulating red blood cells, whereas in normal individuals they are rarely seen and generally account for less than 3%
Blood indices: Elevated mean corpuscular hemoglobin concentration (MCHC) and increased reticulocyte count are common.
Hemolysis screen: Raised bilirubin and LDH, reduced haptoglobin.
Confirmatory tests: Osmotic fragility testing and cation permeability studies may assist, though rarely performed outside reference centres.
Differential diagnoses include hereditary spherocytosis, liver disease–related stomatocytosis, and other red-cell membrane disorders.
Clinical Features:
The symptoms of stomatocytosis can vary depending on the severity of the disorder. In some cases, people with stomatocytosis may not experience any symptoms at all. However, in more severe cases, the following symptoms may occur:
- Fatigue
- Weakness
- Shortness of breath
- Jaundice
- Enlarged spleen
As outlined above, stomatocytes are erythrocytes with a central slit or stoma instead of a circular area of pallor when examined on dried smears; they are uniconcave rather than biconcave, giving them a bowl-like appearance. A few stomatocytes may be observed in blood smears prepared from normal individuals, as well as from patients with acute alcoholism and hepatobiliary disease. Large numbers of stomatocytes are associated with very rare hereditary disorders of red cell cation permeability leading to increased or decreased red cell water content.

Comprehensive diagram of red blood cell morphology illustrating stomatocytes alongside other abnormal RBC shapes.
Hereditary Stomatocytosis comprises two different diseases: the xerocytosis or dehydrated hereditary stomatocytosis and the overhydrated hereditary stomatocytosis. Both are genetic disorders mainly due to an abnormality of red cell membrane permeability to monovalent cations (Na+ and K+) resulting in an alteration in the red blood cell water content. The movement of divalent cations and anions is normal. Typical red blood cells known as stomatocytes (mouth-featured cells) appear in blood smear examination. The clinical manifestation can vary from asymptomatic to severe hemolytic anemia. Hereditary Stomatocytosis shows autosomal dominant inheritance and may cause severe hemolytic anemia presenting very early in life.
Hemolytic anemia with stomatocytosis (up to 40–60%), elevated reticulocyte count, elevated serum bilirubin levels, and reduced serum haptoglobin concentration in children or adolescents are characteristic features of hereditary stomatocytosis.

Peripheral blood film displaying abundant stomatocytes with a distinct central slit, a typical feature of stomatocytosis.
Stomatocytes have been noted in diverse acquired conditions, including neoplasms, cardiovascular and chronic liver disease, alcoholism, and therapy with drugs, some of which are known to be stomatocytogenic in vitro. In some of these conditions, the percentage of stomatocytes on the peripheral blood smear can approach 100%. However, the clinical significance of this observation is unclear because stomatocytes are absent in most patients with the conditions listed. Furthermore, some stomatocytes can be found in normal individuals (3–5%). The most consistent association is that of stomatocytosis and heavy alcohol consumption.
Splenectomy ameliorates anemia in some cases.
Acquired stomatocytosis with hemolytic anemia occurs primarily with recent excessive alcohol ingestion. Stomatocytes in the peripheral blood and hemolysis disappear within 2 weeks of alcohol withdrawal. Stomatocytosis could also be seen in thalassemia, neoplastic, cardiovascular or hepatobiliary disease including acute alcoholism and during therapy with certain drugs some of which are known to be stomatocytogenic in vitro.
Among the common drugs associated with stomatocytogenic effects:
- Hydroxyurea
- Propranolol
- Quinine
- Valproic Acid
- Phenothiazines e.g. chlorpromazine
- Cytosine arabinoside (Ara-C)
- 6-thioguanine
There is no cure for hereditary stomatocytosis, but treatment may be recommended to manage symptoms. This may include blood transfusions, medications to control symptoms, and in severe cases, splenectomy.
Questions and Answers:
What is stomatocytosis and what does a stomatocyte look like?
Stomatocytosis is a red blood cell membrane disorder characterized by erythrocytes with a slit-like central pallor resembling a “mouth.” On a peripheral blood film, stomatocytes appear with elongated or rectangular central pallor, often giving the RBC a uniconcave appearance. The images in the post visually demonstrate this classic slit-like morphology.
What causes hereditary stomatocytosis?
Hereditary stomatocytosis results from mutations in membrane transport proteins, most commonly PIEZO1 and RHAG, leading to abnormal cation permeability. This causes either overhydrated or dehydrated red blood cells, both associated with hemolytic anemia of variable severity.
Which conditions can cause acquired stomatocytosis?
Acquired stomatocytosis is often linked to alcohol use disorder, liver disease, post-transfusion states, and exposure to certain medications such as vinblastine or chlorpromazine. It is usually reversible once the underlying trigger is addressed.
How is stomatocytosis diagnosed on a blood film?
Diagnosis is based on morphological identification of stomatocytes—red cells with a central slit-like pallor—as seen in the provided images. Supportive tests may include osmotic fragility, EMA binding, ektacytometry, and genetic testing in hereditary cases.
What is the difference between hereditary and acquired stomatocytosis?
Hereditary stomatocytosis is caused by membrane channel gene mutations, persistent, and associated with chronic hemolysis. Acquired stomatocytosis is transient and secondary to alcohol, liver disease, or drugs, with resolution once the cause is corrected.
Can stomatocytosis cause hemolytic anemia?
Yes. In hereditary forms, altered cation flux leads to RBC dehydration or overhydration, reduced membrane stability, and chronic hemolysis. Patients may present with jaundice, splenomegaly, reticulocytosis, or gallstones.
Is splenectomy recommended in stomatocytosis?
Splenectomy is generally contraindicated, especially in dehydrated hereditary stomatocytosis, due to a high risk of life-threatening thromboembolic events post-splenectomy. Genetic confirmation helps guide management decisions.
Which laboratory tests help differentiate stomatocytosis from other poikilocytes?
Distinguishing features rely on the slit-like central pallor. Ektacytometry can classify RBC hydration status, while genetic testing confirms PIEZO1 or RHAG variants. The differential includes spherocytes, target cells, ovalocytes, and schistocytes, as illustrated in the morphology diagram.
Does alcohol-induced stomatocytosis resolve?
Yes. In most cases, stomatocytosis related to alcohol use improves within weeks of abstinence as RBC membrane integrity normalizes.
Can stomatocytosis occur in transfused patients?
Yes. Passive transfer of stomatocytes may be seen post-transfusion, representing the donor’s RBC morphology rather than an intrinsic membrane defect in the recipient.
References:
Gallagher PG, Naeim F, Glader B. Red Blood Cell Membrane Disorders. Available from: ScienceDirect.
Red blood cell morphology. Shape of red blood cell. Available from: Adobe Stock.
Neville AJ, Rand CA, Barr RD, Mohan Pai KR. Drug-induced stomatocytosis and anemia during consolidation chemotherapy of childhood acute leukemia. Am J Med Sci. 1984;287(1):3–7. doi:10.1097/00000441-198401000-00001.
Gallagher PG. Red cell membrane disorders. Hematology Am Soc Hematol Educ Program. 2013;2013(1):16–21.
Bruce LJ, Cope DL. Inherited erythrocyte membrane disorders—often overlooked diagnoses. Hematology Am Soc Hematol Educ Program. 2012;2012:461–466.
Andolfo I, Russo R, Iolascon A. Hereditary stomatocytosis: an underdiagnosed condition. Am J Hematol. 2015;90(1):82–86.
Bain BJ. Blood Cells: A Practical Guide. 5th ed. Wiley Blackwell; 2015.
Stewart GW, et al. Mutations in RhAG cause overhydrated hereditary stomatocytosis. Blood. 2011;117(3):1112–1122.
Da Costa L, Mohandas N. Red cell membrane disorders. In: Hoffman R, Benz EJ, Silberstein LE, et al., eds. Hematology: Basic Principles and Practice. 7th ed. Elsevier; 2018. https://www.sciencedirect.com/book/9780323357623/hematology
MedlinePlus Genetics – Hereditary Stomatocytosis. U.S. National Library of Medicine.
https://medlineplus.gov/genetics/condition/hereditary-stomatocytosis/
Keywords:
stomatocytosis, hereditary stomatocytosis, dehydrated hereditary stomatocytosis, overhydrated hereditary stomatocytosis, stomatocyte morphology, red blood cell stomatocytes, stomatocytosis blood smear findings, stomatocytosis diagnosis, stomatocytosis causes, stomatocytosis symptoms, stomatocytosis treatment, acquired stomatocytosis causes, stomatocytosis hemolytic anemia, stomatocytosis gene mutations, PIEZO1 mutations stomatocytosis, RHAG mutations stomatocytosis, red blood cell membrane defects stomatocytosis, RBC dehydration stomatocytosis, stomatocytosis vs normal RBC, RBC morphology stomatocytes, peripheral blood film stomatocytes, Dr Moustafa Abdou, Ask Hematologist






Request Online Consultation With Dr M Abdou
Fee: US$100
Secure payment via PayPal (credit and debit cards accepted)
Pay Now
How do they test for for Stomatocytosis? My 25 year old daughter has a chronic illness Endometriosis stage 4( which has not got the amount of research it should) and she has symptoms of Anemia.. Her hematocrit is 32.5 and hemoglobin is 10.5 and her latest blood test says Stomatocytes are present but no percentage. Most doctors want to blame everything on her Endometriosis but anemia is not a symptom. So we just want to make sure we arent missing anything. Thank you for any information or advice.
Hi Patricia,
Stomatocytes are identified on the blood smear and can be seen in a variety of medical conditions especially liver disease and excess alcohol consumption. I don’t think there is a direct link between endometriosis and stomatocytosis. Anemia associated with endometriosis could be secondary to iron deficiency caused by heavy periods.
BW,
I have had various blood tests and a blood smear test said occasional target cells. Image result for Stomatocytes
Stomatocytes and elliptocytes present. Can you cause this to happen if you work too much, dont sleep enough, or are stressed or dont eat properly, why is my blood test showing this please and what does it mean for me? can it go and turn to a normal blood test again. I dont drink or smoke. Thank you. Michele
Hi Michele,
Thank you for your comment.
Some stomatocytes and elliptocytes can be seen in normal individuals and they don’t have any clinical significance as long as you are not anemic or having chronic liver disease. You can simply ignore them.
BW,
Can i ask what is the possible treatment for the acquired stomatocytes.
Hi,
Thanks for your comment.
The treatment of the acquired stomatocytosis is the treatment of the underlying cause, e.g. liver disease, excessive alcohol ingestion, etc.
BW,
I have had various blood test, and it said i have Silent congenital ovalocytosis and stomatocytosis and reactive leucocytosis.
What is the possible treatment and can it go and turn to a normal blood test again.
Hi Louie,
Thanks for your comment.
At present, there is no specific treatment for Hereditary Stomatocytosis. Many patients with hemolytic anemia take folic acid (vitamin B9) since the greater turnover of cells consumes this vitamin. During crises, transfusion may be required. Unlike hereditary spherocytosis, splenectomy is not indicated.
BW,
I know very little about a childhood blood disorder that may be hereditary stomatocytosis. I recall being told that I could be found eating dirt as a toddler and that I was transfused in the early 1970s. Throughout life (now 53, male), I have either been anemic or on the low end of the normal range and had low iron level readings in blood tests. A year ago, I had iron infusions and took an iron supplement. Energy level and blood test greatly improved. I discontinued the supplement when my iron level was in the upper end of the range (about 9 months ago). Endoscopy was unremarkable. One benign polyp on colonoscopy. No alcohol for three years. Had been a drinker (at times heavy) for 30 years. Stomatocytosis observed by hematologist over last several years. Iron levels falling since discontinuation of supplements. Feeling fatigue and chest tightness that improves with exercise. I have asthma, but I actually breath better the more I exercise. Sleep apnea well controlled with biPAP. I walk 20+ miles a week. Also have Selective IgM deficiency, which makes me very prone to respiratory infections. I live in a humid environment, and lately feel like I just can’t breath. Makes me anxious. Seeing the hematologist for tests again soon. Suspect I have anemia and low iron. No obvious bleeding. Slightly fatty liver, but not awful. Enzymes in normal range. A1C slightly elevated but not diabetic. I do take omeprazole and atorvastatin. Also Symbicort and albuterol. What else should I be asking my doctors? My blood pressure is slightly high, GP wants me to consider medication for that. I want to stay active. Doctors seem puzzled when I say the chest tightness goes away when I’m walking hard. I don’t think it’s asthma, and I did feel really good when I know my iron and hemoglobin were higher.
Hi MW,
Thanks for your comment.
If you have excluded blood loss as a possible cause of your iron deficiency anaemia, I would suggest to also exclude malabsorption of iron from the bowel by checking Anti-endomysial antibody (EMA) and tissue transglutaminase antibody (tTG) levels.
BW,
Hello,
I had a CBC and it showed slight stomatocytes, however, I had a repeat test done three weeks later, but I do not see anything that suggests stomatocytes are still present. What could that mean?
Thank you!
Hi Rose,
Thanks for your comment.
Acquired Stomatocytosis can be found in normal individuals (3–5%).
The most consistent association is between stomatocytosis and chronic liver disease and/or heavy alcohol consumption.
They shouldn’t cause concern if the blood indices are normal and you are not anemic.
BW,
Thank you very much for your response.
You’re welcome!
Hello.
I have been told that I have MDS following blood tests done after a GI bleed. The blood test results showed: RBC 3.81 – MCV 103.6 – MCH 35.2 – PLATELETS 91.
Blood tests showed macrocytosis with stomatocytes present.
Doctor says that I have MDS.
Bone marrow biopsy results showed ? fingerprinting film in both liquid and ‘hard’ marrow test of lymphocytes being present?
Alcohol intake really quite low.
Non smoker for 25 years.
Low platelet count has been present for 30 years following a massive viral infection acquired whilst on holiday in the Gambia resulting in 6 months of work. (unheard of to take time off work for me)
Was contacted by the NHS following a visit to the hotel in London at the same time that the Russian ‘spy’ was in contact with polonium poisoning????
Any comments would be gratefully accepted please.
Hi Lesley,
Thank you for reaching out. I understand your concern about the MDS diagnosis.
To provide a more accurate assessment, I would need to review the complete bone marrow biopsy report.
Additionally, it’s important to rule out other potential causes of macrocytosis such as B12/Folate deficiency, liver disease, and underactive thyroid.
Please send me the complete report so that I can assist you further.
Your long-standing low platelets could be immune-mediated or drug-related.
BW,
I have had stomacytosis for over a year, but recently discovered my phosphorous has been around 2 or less as well. Extreme fatigue, bone weakness, kidney stones, confusion, brain fog, spleen calcifications, tinnitus and straightening of the cervicel lordosis
My coworker who’s a doctor sees I bring Diet Coke everyday to work and prescribed me phosphate 250 drug. I am confused how a drink that has phosphoric acid can deplete my phosphorus and also cause stomacytosis. I just started it today and I am hoping this will fix my chronic fatigue and brain fog. I switched to light colored diet sodas instead.
Just haven’t seen much online about this Diet Coke and low phos and stomacytosis problem. And been hunting a year for this problem with no answers till recently.
I feel alone in this problem as I haven’t seen others talk about this, was wondering if you have seen anything similar?
Hi Tora,
I’m sorry to hear about your health challenges. It’s understandable that you’re feeling confused and frustrated.
As is well known, cola represents a strong exogenous source of phosphate, due to its high phosphorus content (about 15–20 mg/dL), more than other carbonated soft drinks. High consumption of cola can cause a sudden change in the pH gastric values as a consequence of the strong cola acidity (pH 1.8). The effect of cola on calcium concentration seems to be connected to its high phosphate concentration. Indeed, when the cola drink is ingested, a considerable decrease in calcium concentration and, of course, an increase in phosphorus concentration is observed.
However, I don’t think there is a direct link between cola consumption and stomatocytosis. If you don’t drink alcohol in excess, I would suggest checking your liver function tests, including gamma GT, and having an ultrasound scan on your liver.
BW
Dr. M Abdou
Hello; My wife passed away. But, at first, doctors thought she had cirrhosis. Although her LFTs were normal, she had a high Total Bilirubin, and Normal direct billi, with slightly low albumin. A liver biopsy showed Fatty liver, 1 of 3 ballooning, and grade 1 fibrosis.
She had gone into the hospital with a bleed from Eshphugeal erosion caused by bile reflux. For one reason or another, they treated her with 2g of Cefraxone and 1g of Vancomycin. She developed a severe AKI and had to be admitted.
They then ran into issues, that she needed a blood transfusion every 4-5 days. A GI scope found no bleeds, a colonoscopy found no bleeds, and stool testing showed no blood present.
Her Albumin levels were bouncing all over the planet from normal to low back to normal to low. One day it would be normal the next below normal, a few days later. Back up again.
Blood Smears showed a high level of Stomatocytes and Polychromasia. Her liver was slightly enlarged at 15.6 cm. Spleen Normal, Dopler showed normal portal flow.
Her ammonia levels were normal.
Could the Hemolysis going on be a reaction to the Cefraxone?
She died due to Renal failure from a toxic vancomycin trough level of 86.8.
Hi Charles,
I extend my deepest condolences for the loss of your wife.
I appreciate you reaching out, and I understand the importance of clarifying the circumstances surrounding her passing.
It’s crucial to consider the complexities involved in such cases.
Immune hemolytic anemia can indeed be a rare adverse effect of medications like ceftriaxone and vancomycin.
However, implicating them directly requires a thorough assessment of the clinical context.
Regarding vancomycin-induced acute kidney injury (AKI), although many cases are reversible, the association with a higher incidence of end-stage kidney disease and increased mortality rates underscores the need for a careful evaluation of the overall clinical picture.
The presence of stomatocytes and polychromasia in the blood raises concerns about potential liver disease and the release of immature red blood cells from the bone marrow (reticulocytes) due to hemolysis or blood loss. Performing a direct Coombs test as part of routine investigations is a prudent step to differentiate between immune and non-immune hemolysis, which might be contributory to the elevated indirect bilirubin in your wife’s case.
Given the complexity of the situation, it is challenging to draw definitive conclusions based solely on the information provided. The differential diagnosis should include considerations of microangiopathic hemolytic anemia (MAHA) which carries a poor prognosis.
Best regards,
Dr. M Abdou