Transfusion Medicine

Transfusion Medicine is a vital specialty focused on the transfusion of blood and its components. This field is incredibly broad, encompassing every aspect from blood donation and blood banking to advanced practices like therapeutic apheresis, stem cell collection, and cellular therapy. In the lab, blood banking ensures all donated blood and blood products are safe for use by performing essential tests, including blood typing (immunohematology) and screening for infectious diseases. Understanding this comprehensive process is key to modern medical care and ensuring patient safety.
According to the American Association of Blood Banks as of 2013:
About 36,000 units of blood are needed every day.
The number of blood units donated is about 13.6 million a year.
About 6.8 million volunteers are blood donors each year.
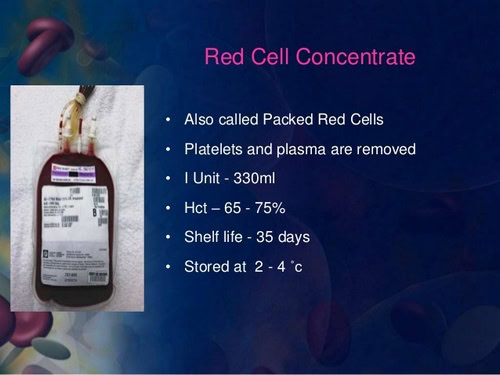
Each unit of blood is broken down into components, such as red blood cells, plasma, cryoprecipitated AHF, and platelets. One unit of whole blood, once it’s separated, may be transfused to several patients, each with different needs.
Annually, more than 21 million blood components are transfused.
Who are the blood donors?
Most blood donors are volunteers. However, sometimes, a patient may want to donate blood a couple of weeks before undergoing surgery, so that his or her blood is available in case of a blood transfusion. Donating blood for yourself is called an autologous donation. Volunteer blood donors must pass certain criteria, including the following:
- Must be at least 16 years of age, or in accordance with state law.
- Must be in good health.
- Must weigh at least 50 kilograms.
- Must pass the physical and health history exam given before donation.
- Some states permit people younger than 16 or 17 years to donate blood, with parental consent.
What tests are done in blood banking?
A certain set of standard tests are done in the lab once blood is donated, including, but not limited to, the following:
Typing: ABO group (blood type).
Rh typing (positive or negative antigen).
Screening for any unexpected red blood cell antibodies that may cause problems in the recipient.
Screening for current or past infections, including:
- Hepatitis viruses B and C
- Human immunodeficiency virus (HIV)
- Human T-lymphotropic viruses (HTLV) I and II
- Syphilis
- West Nile virus
- Chagas disease
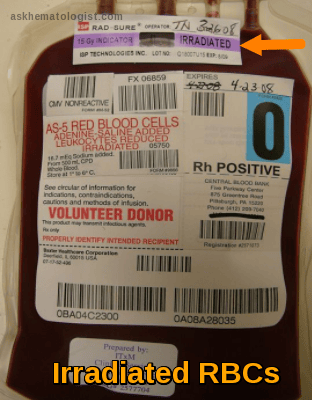
Irradiation to blood cells is performed to disable any T-lymphocytes present in the donated blood (T-lymphocytes can cause a reaction when transfused, but can also cause graft-versus-host problems with repeated exposure to foreign cells). Transfusion-associated graft versus host disease (TA-GvHD) is a rare but almost lethal complication of blood transfusion in immunocompromised patients. To prevent TA-GvHD, irradiated blood products should be given to patients at risk: patients after bone marrow transplantation, newborns and children in the 1st year, patients with severe combined immunodeficiency, and patients receiving blood from first-degree relatives.
Patients treated with purine analogue drugs (Fludarabine, Cladribine, and deoxycoformycin) should receive irradiated blood components indefinitely. The situation with other purine analogues such as Bendamustine and clofarabine is unclear, but the use of irradiated blood components is recommended as these agents have a similar mode of action. Irradiated blood components should be used after alemtuzumab (anti- CD52) therapy.
Cellular blood components are irradiated by either X-ray or irradiation and are identified by an approved overstick label which should include the date of irradiation and any reduction in shelf life. The minimum dose achieved in the irradiation volume should be 25Gy, with no part receiving more than 50Gy.
Red cells may be irradiated at any time up to 14 days after collection, and thereafter stored for a further 14 days from irradiation. Where the patient is at particular risk from hyperkalemia, e.g. intrauterine or neonatal exchange transfusion, it is recommended that red cells be transfused within 24 hrs of irradiation or cells are washed.
Platelets can be irradiated at any stage during storage and can thereafter be stored up to their normal shelf life after collection.
Granulocytes for all recipients should be irradiated before issue, and thereafter transfused with minimum delay.
Irradiated components not used for the intended recipient can be safely returned to stock to be used for recipients who do not require irradiated components. The reduction in shelf life must be observed.
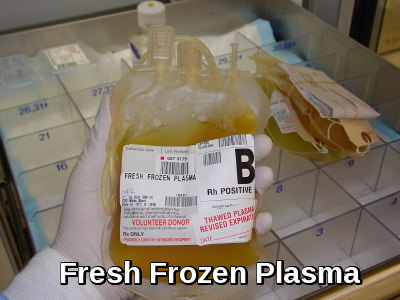
It is not necessary to irradiate fresh frozen plasma, cryoprecipitate or fractionated blood products.
Leukocyte-reduced blood has been filtered to remove the white blood cells that contain antibodies that can cause fevers in the recipient of the transfusion (These antibodies, with repeated transfusions, may also increase a recipient’s risk of reactions to subsequent transfusions).
What are the blood types?
According to the American Association of Blood Banks, distribution of blood types in the U.S. includes the following:
- O Rh-positive – 39%
- A Rh-positive – 31%
- B Rh-positive – 9%
- O Rh-negative – 9%
- A Rh-negative – 6%
- AB Rh-positive – 3%
- B Rh-negative – 2%
- AB Rh-negative – 1%
What are the components of blood?
While blood, or one of its components, may be transferred, each component serves many functions, including the following:
Red blood cells: These cells carry oxygen to the tissues in the body and are commonly used in the treatment of anemia.
Platelets: They help the blood to clot and are used in the treatment of leukemia and other forms of cancer.
White blood cells: These cells help to fight infection, and aid in the immune process.
Plasma: The watery, liquid part of the blood in which the red blood cells, white blood cells, and platelets are suspended. Plasma is needed to carry the many parts of the blood through the bloodstream. Plasma serves many functions, including the following:
- Helps to maintain blood pressure.
- Provides proteins for blood clotting.
- Balances the levels of sodium and potassium.
Cryoprecipitate AHF: The portion of the plasma that contains clotting factors that help to control bleeding.

Albumin, immune globulins, and clotting factor concentrates: may also be separated and processed for transfusions.
What is a blood transfusion?

A blood transfusion is a procedure in which you receive blood or parts of blood through an IV (intravenous) line. The blood may be from a donor. Or you may receive your own blood that has been stored for you. There are several parts of blood that can be transfused into an adult. Red blood cells are the most common type of blood product transfusion.
Why might I need a blood transfusion?
There are several reasons why you may need a blood transfusion, such as:
- A sudden loss of blood due to an accident or injury.
- Blood loss as a result of surgery.
- A low hemoglobin level before, during, or after surgery.
- Severe heart, lung, liver, or kidney disease.
- Bone marrow failure.
- Moderate to severe anemia (decreased red blood cells).
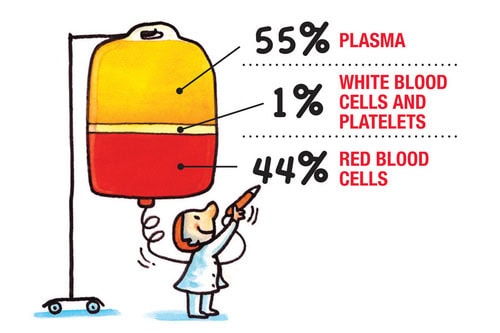
The parts of blood:
Human blood is made of a fluid called plasma. Plasma carries red and white blood cells and platelets. Each part of blood has a special function. These parts can be separated from each other. Bone marrow, the soft, spongy material in the center of the bones, makes most of the body’s blood cells.
Here is a look at each part of the blood, and why it might be transfused:
Red blood cells: These cells carry oxygen from your lungs to other body organs. They also carry carbon dioxide back to the lungs to be breathed out (exhaled). The body needs a certain number of these cells to work well. Bleeding due to injury, surgery, or disease may cause a low red blood cell count. This is the most common type of transfusion.
White blood cells: These cells fight infections by destroying bacteria, viruses, and other germs. White blood cells are rarely transfused. They are often set aside as a short-term (temporary) treatment for people with a low white cell count and severe infection that has not responded to antibiotics.
Platelets: These little pieces of blood cells help blood to clot. Your body may not make enough platelets. This might be due to bone marrow disorders, increased destruction of platelets, or medicines such as chemotherapy. Platelets may be transfused before a procedure that may cause a person with a low platelet count to bleed.

Plasma: This fluid carries the blood cells all over the body. It contains proteins, vitamins, and minerals. Some of the proteins also help blood to clot. Plasma or fresh frozen plasma can be transfused in people who severely lack certain parts of the blood that help with clotting.
What are the risks of a blood transfusion?
Most hospitals use blood from volunteer donors. These donors are not paid for giving blood or blood products. Each blood donor must answer medical history questions and have a limited physical exam before being accepted as a donor. Donated blood is carefully tested, which lowers the chances of transfusion-related infections.
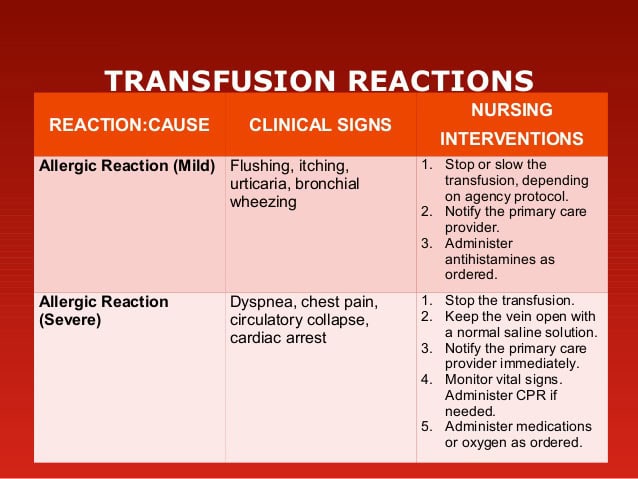
Transfusion reactions can occur even if the donated blood is the right blood type. Transfusion with blood that is the wrong type can be fatal. But this is unlikely to occur because medical workers check blood multiple times.
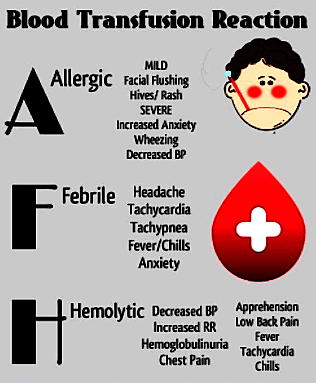
The most common complications of transfusion are:
- Febrile nonhemolytic reactions.
- Chill-rigor reactions.
The most serious complications, which have very high mortality rates, are:
- Transfusion-associated circulatory overload.
- Transfusion-related acute lung injury.
- Acute hemolytic reaction due to ABO incompatibility.
Early recognition of symptoms suggestive of a transfusion reaction and prompt reporting to the blood bank is essential. The most common symptoms are chills, rigor, fever, dyspnea, light-headedness, urticaria, itching, and flank pain. If any of these symptoms (other than localized urticaria and itching) occur, the transfusion should be stopped immediately and the IV line kept open with normal saline. The remainder of the blood product and clotted and anticoagulated samples of the patient’s blood should be sent to the blood bank for investigation. Note: The unit in question should not be restarted, and transfusion of any previously issued unit should not be initiated.Further transfusion should be delayed until the cause of the reaction is known, unless the need is urgent, in which case type O Rh-negative RBCs should be used.
Hemolysis of donor or recipient RBCs (usually the former) during or after transfusion can result from ABO/Rh incompatibility, plasma antibodies, or hemolyzed or fragile RBCs (eg, by overwarming stored blood or contact with hypotonic IV solutions). Hemolysis is most common and most severe when incompatible donor RBCs are hemolyzed by antibodies in the recipient’s plasma. Hemolytic reactions may be acute (within 24 h) or delayed (from 1 to 14 days).
Most febrile reactions are treated successfully with acetaminophen and, if necessary, diphenhydramine. Patients should also be treated (eg, with acetaminophen) before future transfusions. If a recipient has experienced more than one febrile reaction, special leukoreduction filters are used during future transfusions; most hospitals use prestorage, leukoreduced blood components.
Delayed hemolytic transfusion reactions (DHTRs) occur in patients who have received transfusions in the past. These patients may have very low antibody titers that are undetectable on pretransfusion testing, so that seemingly compatible units of red blood cells (RBCs) are transfused. Exposure to antigen-positive RBCs then provokes an anamnestic response and increased synthesis of the corresponding antibody. After several days, the antibody titer becomes high enough to hemolyze transfused RBCs. The frequency of DHTRs is estimated to be approximately 1 case per 5400 red cell units transfused.
Other types of blood donation:
In addition to general volunteer blood donations, there are 2 other types of blood donation:
Directed blood donation: This is when friends or family donate blood for a certain person. This blood is set aside for that person’s use. This type of donation requires a prescription and must be scheduled in advance. Direct blood donations go through the same testing as other volunteer donations. If the person does not use this donated blood, it may be made available for someone else.
Donating blood for yourself (autologous donation): This is your blood that you donate for your own use. It is set aside and can be transfused back into your own body if needed for a later, planned surgery. This type of donation requires a prescription from your provider and is scheduled in advance. It does not go through the same testing as other blood donations. If you don’t use the blood, it is thrown away.
How do I get ready for a blood transfusion?
No special preparation is needed before a blood transfusion.
What happens during a blood transfusion?
A blood transfusion may occur as part of your hospitalization. Or it may be done as an outpatient. This means you go home the same day.
Blood is collected and stored in germ-free (sterile) bags. The bags are used once and then thrown away.
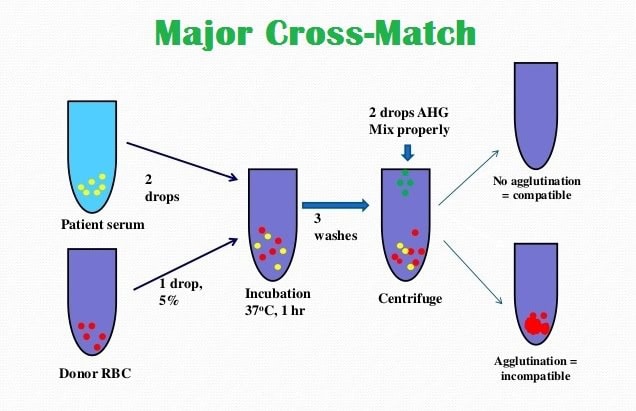
Before blood is given to you, it is crossmatched with your own blood to make sure it is compatible.
The blood will be given through a needle or thin tube (catheter) placed in a vein.
Your temperature, blood pressure, and heart rate will be checked many times while the blood is being given. It may take a few hours to complete the process.
What happens after a blood transfusion?
After you have received the blood as requested by your healthcare provider, the IV that was placed in your arm will be removed and you will be discharged. You will be able to go back to your normal activities unless your healthcare provider has made other recommendations.
References:
Johns Hopkins Medicine. Blood Donations and Blood Banking. Johns Hopkins Medicine Health Library.
Johns Hopkins Medicine. Blood Transfusions – Indications, Types, and Risks. Johns Hopkins Medicine Health Library.
Effie Grand. Department of Haematology, Salisbury NHS Foundation Trust. Irradiation of Blood Components – Clinical Guidelines. ICID Salisbury NHS.
Ravindra Sarode, MD. Complications of Transfusion. Hematology and Oncology – MSD Manual Professional Edition. MSD Manual.
S. Gerald Sandler, MD, FACP, FCAP. Transfusion Reactions: Practice Essentials, Background, Pathophysiology. Medscape Reference.
AABB (American Association of Blood Banks). Standards for Blood Banks and Transfusion Services, 33rd Edition. AABB Press, Bethesda, MD; 2024.
British Society for Haematology (BSH). Guidelines on the Administration of Blood Components. Br J Haematol. 2020; 191(6): 703–726. doi:10.1111/bjh.16922.
World Health Organization (WHO). Blood Safety and Availability. WHO Factsheet.
Centers for Disease Control and Prevention (CDC). Transfusion-Transmitted Infections – Epidemiology and Prevention. CDC Transfusion Safety.
Carson JL, Guyatt G, Heddle NM, et al. Clinical Practice Guidelines from the AABB: Red Blood Cell Transfusion Thresholds and Storage. JAMA. 2016; 316(19): 2025–2035. doi:10.1001/jama.2016.9185
Keywords:
Transfusion Medicine, Blood Transfusion, Blood Banking, Blood donation, Autologous donation, Blood components, Directed blood donation, Therapeutic apheresis, Blood safety testing, Blood typing, ABO blood type, Rh typing, Blood screening, Irradiated blood components, Leukocyte-reduced blood, Red blood cells transfusion, Platelets transfusion, Plasma transfusion, Cryoprecipitate AHF, Blood transfusion risks, Transfusion reactions, TRALI, Acute hemolytic reaction, Complications of blood transfusion, Ask a hematologist about blood transfusions

Related Posts:




Request Online Consultation With Dr M Abdou
Fee: US$100
Secure payment via PayPal (credit and debit cards accepted)
Pay Now
That’s an interesting idea to have some of your own blood taken to be replaced later. I could see how that would be a good way to make sure you have a blood type match if you are planning in losing blood from surgery or something. That would be cool if you could do that to help replace your white blood cells and other parts of your blood as well.